


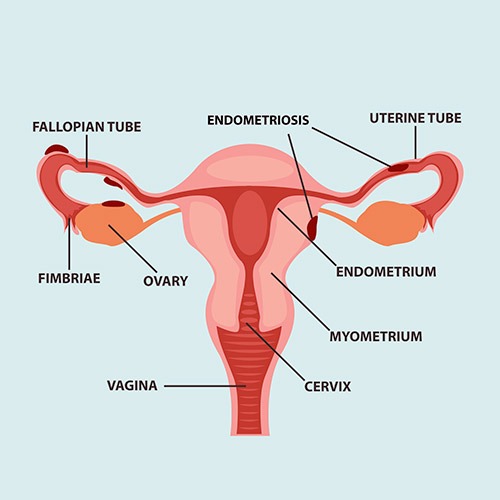
Endometriosis
The endometrium is the tissue that covers the uterine cavity just like a carpet where the embryo will be implanted. Endometriosis is a condition in which tissue identical to the uterine wall (endometrium) is detected out of the uterus, particularly in the pelvic cavity. This tissue can develop in organs such as the ovaries, the uterus, the intestinal and pelvic walls causing inflammation and pain.
During each cycle, when an egg is not fertilized and no implantation or pregnancy occur, the inner lining of the uterus is rejected by bleeding through the vaginal cavity (period or menstruation). But in case the wall outside the uterus is ruptured, blood cannot leave the body, thus creating inflammation and pain. Endometriosis can affect women physically, socially and also mentally. The most common symptoms are dysmenorrhea and painful ovulation, abnormal bleeding, pain during or after sexual intercourse, abdominal pain, fatigue and possibly infertility.
About 10% of women in childbearing age present endometriosis symptoms and a 30-40% of them may never be able to have children. Moreover, 50% of infertile women suffer from endometriosis. At present there is no known cure for endometriosis and the diagnosis becomes laparoscopically. It is noteworthy that once you start experiencing the first symptoms, it takes an average of 8.5 years until the full diagnosis.
Adenomyosis is a pathological condition where endometrial tissue penetrates the wall of the uterus. It occurs in women of reproductive age and is a benign disease. Sometimes there are symptoms such as pain in the period (dysmenorrhea), increase blood flow during period and also increased uterine size. Various theories have been put forward regarding adenomyosis such as genetic factors associated with the uterine development of the fetus during the first months of pregnancy.
Others consider the breakage of the layer between the endometrium and myometrium during surgery allows penetration of endometrial cells in the myometrium. Recently the cutting-edge technology of 3D ultrasound and MRI allows us to confirm the existence of adenomyosis.
The above painless imaging methods in combination with histopathology help us categorize adenomyosis into 2 categories: the focal with an organized benign tumor appearance (adenomyoma) and the diffuse.
Women with adenomyosis tend to show an increased rate of infertility and miscarriages compared with women of the same age and same reproductive profiles in general. This is due to alterations of the microenvironment of the womb which is no more receptive to embryo implantation. Regarding miscarriages, they are mainly related to changing hormonal factors and disturbed microcirculation of the endometrial cavity.
Thus, the fertility specialist should highlight the existence of adenomyvosis of the infertile couple and formulate an appropriate strategy in order to achieve pregnancy in the shortest possible time.
The approach may be pharmaceutical, surgical – laparoscopic or even just waiting, i.e. in the case of a young infertile couple without other coexisting factors, waiting and monitoring could possibly bring the desired results.
The existence of adenomyosis coexists in the majority of cases with endometriosis. Both endometriosis and adenomyosis still remain a medical riddle about their pathophysiological mechanism and have not been fully elucidated. Manipulations of infertile couples should be meticulous since we aim at obtaining the best possible result.
We are here to answer any questions and discuss with you.
a

